Microbyte-Pathogen Series: Ureaplasma urealyticum: Urea Metabolism and Reproductive Complications
Introduction
The human urogenital tract hosts a complex ecosystem of microorganisms, among which Ureaplasma urealyticum stands out as a unique and clinically significant bacterial species. Belonging to the class Mollicutes, this fastidious bacterium is characterized by its exceptionally small size and the complete absence of a rigid peptidoglycan cell wall. While it frequently exists as a harmless commensal organism within the reproductive tract of sexually active adults, it is an opportunistic pathogen capable of causing distinct inflammatory diseases under favorable physiological conditions. Understanding the balance between benign colonization and active infection is a critical challenge in modern clinical microbiology and venereology.
The clinical importance of Ureaplasma urealyticum has gained widespread recognition due to its direct implication in non-gonococcal, non-chlamydial urethritis in men, as well as several adverse reproductive outcomes in women. Furthermore, its ability to undergo vertical transmission introduces severe health risks to newborns, including low birth weight, systemic inflammatory responses, and chronic respiratory complications. As antimicrobial resistance continues to evolve globally, a detailed understanding of this atypical pathogen’s profile, disease-causing mechanisms, diagnostic modalities, and targeted therapeutic strategies is essential for healthcare providers and clinical researchers alike.
What is Ureaplasma urealyticum?
Ureaplasma urealyticum is a unique, minimal bacterium belonging to the class Mollicutes that lacks a cell wall and primarily colonizes the human urogenital mucosal surfaces as an opportunistic pathogen. Due to its lack of a rigid outer wall, it exhibits a highly flexible, pleomorphic structure and is structurally bounded only by a trilayered cytoplasmic membrane containing sterols. It possesses one of the smallest genomes among self-replicating organisms, containing approximately 0.75 to 1.0 megabases, which drastically limits its biosynthetic capabilities and forces it to rely heavily on its host for essential nutrients.
The clinical significance of this organism is deeply tied to its opportunistic nature. In many individuals, Ureaplasma urealyticum resides asymptomatically within the vagina, cervix, or urethra without inducing an inflammatory response. However, when the host immune system is compromised, or when the local microenvironment experiences disruptions (such as shifts in pH or alterations in the surrounding microbiome), the bacterium multiplies rapidly. This overgrowth triggers localized cellular damage and an inflammatory cascade, culminating in symptomatic urogenital tract infections, reproductive complications, and perinatal pathologies.
Taxonomic Classification
Microbe Profile
How Was Ureaplasma urealyticum Discovered and Named?
Ureaplasma urealyticum was discovered in 1954 by Maurice Shepard as a "T-strain" mycoplasma isolated from patients with urethritis and was later named to reflect its singular biochemical property of urea metabolism. Shepard originally recovered these organisms from the urethral exudates of male patients suffering from non-gonococcal urethritis. He designated them as "T-strains" because they produced exceptionally small, microscopic colonies on solid agar media often measuring less than 15 to 30 micrometers in diameter, which were vastly smaller than the typical "fried-egg" colonies generated by conventional Mycoplasma species.
The evolution of its nomenclature represents a vital milestone in modern clinical microbiology. For two decades following its initial isolation, the bacterium remained informally categorized within the genus Mycoplasma. However, in 1974, researchers proposed the creation of a brand-new genus, Ureaplasma, to accommodate these organisms due to their unique, non-typical capacity to generate energy through the breakdown of urea. Modern molecular taxonomy, fueled by advanced comparative genomics and 16S rRNA gene sequencing, subsequently established the clear delineation between Ureaplasma urealyticum and Ureaplasma parvum, cementing U. urealyticum as a distinct pathogen associated with explicit urogenital and perinatal complications.
How Does Ureaplasma urealyticum Cause Disease?
Ureaplasma urealyticum causes disease by utilizing surface adhesins to attach to host epithelial cells and using its potent urease enzyme to generate cytotoxic ammonia, which triggers mucosal inflammation and tissue damage. The pathogenic process is multifactorial, relying on a sophisticated balance of mechanical adherence, metabolic byproduct generation, and host immune system evasion. Because the bacterium resides directly on the mucosal surfaces of the urogenital and respiratory tracts, its virulence factors act directly upon vulnerable host cell membranes.
The cornerstone of its pathogenesis is the production of the intracellular enzyme urease. This enzyme catalyzes the rapid hydrolysis of urea into ammonia ($NH_3$) and carbon dioxide. The localized accumulation of free ammonia generates significant cytotoxicity, elevating the regional microenvironmental pH and directly altering host epithelial cell membrane integrity. This alkaline shift causes cell vacuolation, halts ciliary movement in mucosal linings, and facilitates further bacterial colonization. Concurrently, the bacterium utilizes its Multiple Banded Antigen (MBA) to attach firmly to host cells, while undergoing rapid phase and antigenic variation to escape detection by host immunoglobulins. Furthermore, the activation of host Toll-like receptors (primarily TLR1, TLR2, and TLR6) by bacterial lipoproteins triggers a massive influx of pro-inflammatory cytokines, driving chronic local inflammation and tissue sloughing.
Step-by-Step Pathogenesis
Adhesion and Attachment: The bacterium utilizes specialized surface proteins and the Multiple Banded Antigen (MBA) to bind tightly to the receptors of host urogenital epithelial cells.
Colonization:Ureaplasma urealyticum establishes microcolonies along the mucosal borders, drawing necessary cholesterol and nutrients directly from host cell membranes.
Urease Activation and Ammonia Production: Intracellular urease breaks down host urea, liberating high concentrations of toxic free ammonia into the local cellular environment.
Epithelial Cell Injury: Elevated ammonia levels cause direct cytotoxicity, inducing cellular swelling, vacuolation, and disruption of tight junction barriers.
Immune Evasion: The organism secretes targeted IgA proteases to cleave host secretory antibodies, while altering its surface MBA structure to evade humoral immune defenses.
Biofilm Matrix Production: The bacterial population synthesizes an extracellular polymeric substance (EPS) matrix, building a protective biofilm that shields the colonies from host immune cells and exogenous antibiotics.
Inflammatory Response Amplification: Host pattern recognition receptors detect bacterial lipoproteins, stimulating the continuous release of pro-inflammatory cytokines (such as IL-1β, IL-6, and TNF-α) that damage surrounding tissue.
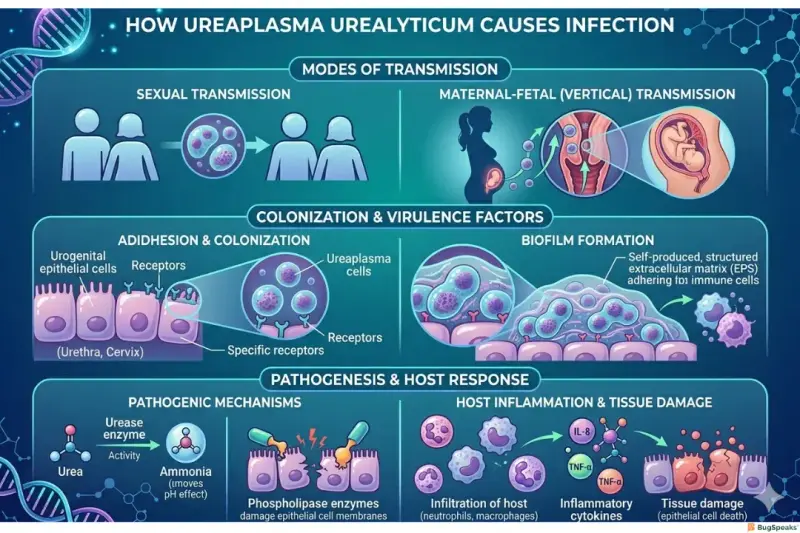
How Is Ureaplasma urealyticum Transmitted?
Ureaplasma urealyticum is transmitted primarily through direct sexual contact between adults or vertically from an infected mother to her offspring during gestation or childbirth. Horizontal transmission among adults is highly correlated with sexual activity, with colonization rates rising progressively alongside an increase in the number of lifetime sexual partners. The organism is transmitted through exchange of infected vaginal fluids, semen, and direct contact with mucosal membranes of the urethra or cervix.
Vertical transmission represents a major clinical concern in maternal-fetal medicine. The bacterium can ascend from the lower maternal genital tract into the uterine cavity, penetrating intact or ruptured fetal membranes to cause chorioamnionitis and infect the amniotic fluid. Additionally, perinatal transmission occurs frequently during childbirth as the neonate passes through an infected birth canal, leading to the colonization of the infant’s skin, nasopharynx, or respiratory tract. It is essential to differentiate between benign colonization, where the organism resides harmlessly as part of the normal adult microbiome, and true active infection, which is defined by tissue invasion and an induced inflammatory state.
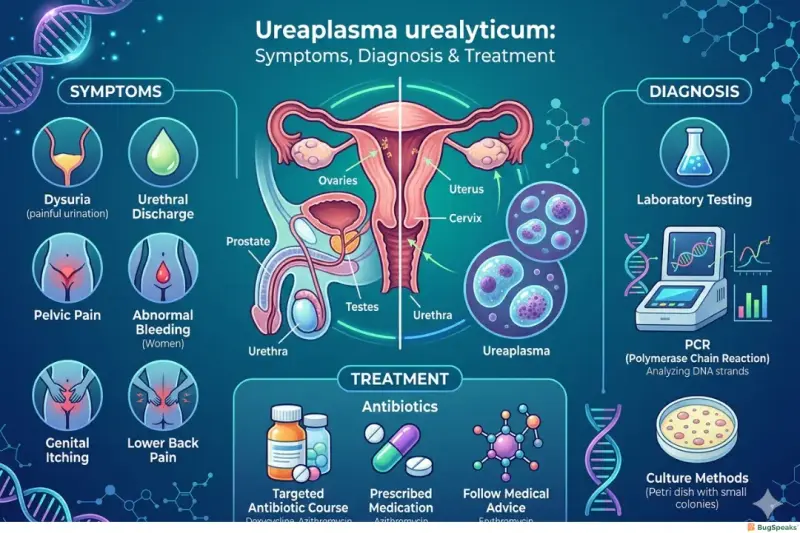
What Are the Signs and Symptoms of Ureaplasma urealyticum Infection?
The signs and symptoms of Ureaplasma urealyticum infection vary from complete absence in asymptomatic individuals to localized burning, discharge, pelvic pain, and severe neonatal respiratory distress. Because the organism has low inherent virulence, many individuals remain completely asymptomatic carriers for extended periods. However, when an active infection develops, the clinical manifestations depend entirely on the patient's age, sex, and anatomical site of colonization.
Symptoms in Women
In women, symptomatic infections present with localized inflammatory conditions of the lower and upper reproductive tract. Common clinical presentations include:
Dysuria (painful or burning sensations during urination)
Abnormal vaginal discharge with altered consistency or odor
Pelvic discomfort or deep-seated lower abdominal pain
Post-coital bleeding or intermenstrual spotting due to cervicitis
In severe ascending cases, signs of pelvic inflammatory disease (PID) or endometritis
Symptoms in Men
In men, the bacterium acts as a principal cause of non-gonococcal, non-chlamydial urethritis (NGNCU). Symptoms usually include:
Watery, mucoid, or clear urethral discharge
Urethral pruritus (itching or tingling sensations inside the penis)
Dysuria and increased urinary frequency
Testicular tenderness or dull aching pain, indicative of secondary epididymitis
Symptoms in Newborns
Neonates infected via vertical or perinatal pathways display structural and systemic symptoms that can be life-threatening. These include:
Neonatal pneumonia and severe respiratory distress syndrome
Cough, tachypnea, and structural abnormalities on chest X-rays (associated with bronchopulmonary dysplasia)
Lethargy, poor feeding, and temperature instability resulting from neonatal sepsis
Neurological signs, including irritability or seizures, caused by Ureaplasma-induced meningitis
Asymptomatic Colonization
A vast segment of the sexually active human population exhibits asymptomatic colonization, harboring Ureaplasma urealyticum within the normal vaginal or urethral flora without any signs of tissue injury. In these instances, the host immune response successfully restrains the bacterial population, keeping it at a low density that does not trigger mucosal inflammation. As a result, finding the bacterium during routine diagnostic workups does not automatically indicate an active disease state.
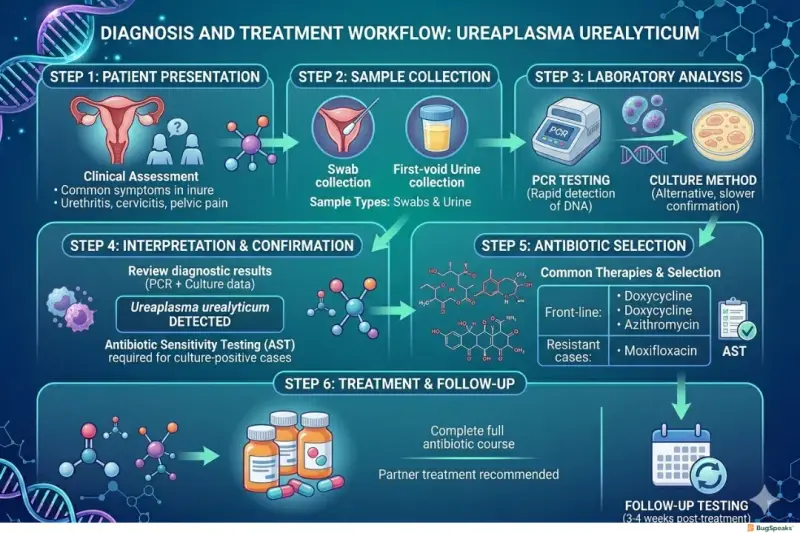
How Is Ureaplasma urealyticum Diagnosed?
Ureaplasma urealyticum is diagnosed using high-sensitivity molecular assays such as Polymerase Chain Reaction (PCR) and Nucleic Acid Amplification Tests (NAATs), as traditional culture is slow and standard Gram staining is ineffective. Because the organism lacks a cell wall, standard light microscopy and traditional Gram staining cannot visualize it. Therefore, diagnosis depends on specialized laboratory modalities capable of identifying either the live organism or its genetic material.
Clinical assessment begins with targeted specimen collection, utilizing urethral, vaginal, or cervical swabs, or first-void urine samples from adult patients. In neonatal cases, endotracheal aspirates, cerebrospinal fluid (CSF), or blood samples are preferred. Traditional culture techniques require specialized liquid or solid media containing urea and horse serum (such as U9 broth or A7/A8 agar). While culture can confirm viability and allow for antibiotic susceptibility testing, it is technically demanding and takes 2 to 5 days. Conversely, NAATs and PCR assays have emerged as the modern diagnostic gold standard. These molecular platforms provide rapid turnaround times, superior sensitivity, and the precise ability to differentiate Ureaplasma urealyticum from Ureaplasma parvum, which is vital for directing appropriate clinical care.
What Treatments Are Available for Ureaplasma urealyticum?
Treatments available for Ureaplasma urealyticum are restricted to specific protein synthesis and DNA replication inhibitors, namely tetracyclines, macrolides, and fluoroquinolones, because the lack of a bacterial cell wall renders all beta-lactam antibiotics entirely obsolete. Standard antibiotics like penicillins, cephalosporins, and vancomycin target cell wall peptidoglycan synthesis, making them ineffective against cell-wall-deficient mollicutes. Consequently, targeted therapies must utilize agents that penetrate the cell membrane to disrupt essential intracellular processes.
Tetracyclines, particularly doxycycline, are traditionally preferred as first-line therapies for uncomplicated urogenital infections due to their strong tissue penetration and consistent efficacy. Macrolides, such as azithromycin, serve as standard alternatives, particularly for pregnant patients or individuals with tetracycline intolerances, given their favorable safety profile. Fluoroquinolones, including moxifloxacin or levofloxacin, are reserved for refractory cases or infections caused by multidrug resistant strains.
Alarming increases in antimicrobial resistance present a growing challenge. Strains harboring the tet(M) gene display high resistance to tetracyclines, while specific mutations within the 23S rRNA gene or ribosomal proteins L4 and L22 lead to macrolide resistance. Clinical treatment decisions must increasingly adapt to local resistance patterns.
How Can Ureaplasma urealyticum Infection Be Prevented?
Ureaplasma urealyticum infection can be prevented by maintaining consistent barrier contraceptive usage, implementing targeted screening during pregnancy, and identifying and treating sexual partners concurrently. Because this bacterium is widely distributed across the human population and is often transmitted sexually, prevention strategies focus on behavioral modifications, early identification, and breaking the cycle of horizontal and vertical transmission.
Practicing safe sex through the consistent use of latex or polyurethane condoms significantly reduces the risk of horizontal transmission by blocking direct mucosal exposure to infected secretions. In clinical and maternal settings, screening considerations focus on symptomatic individuals or pregnant women showing early signs of preterm labor or unexplained chorioamnionitis. When an active infection is diagnosed, managing sexual partners concurrently is essential; both partners must complete the designated antibiotic regimen and abstain from unprotected intercourse to prevent immediate reinfection.
Reference
Waites KB, Katz B, Schelonka RL. Mycoplasmas and Ureaplasmas as neonatal pathogens. Clin Microbiol Rev. 2005;18(4):757-789.
Horner P, Dhasmana D, Cochran K, et al. Is Ureaplasma urealyticum a cause of nongonococcal urethritis? A systematic review and meta-analysis. Clin Infect Dis. 2014;58(9):1284-1292.
Kokkayil P, Dhawan B. Ureaplasma: current perspectives. Indian J Med Microbiol. 2015;33(2):205-214.
Beeton AM, Zhang L, Chaloner C, et al. Antimicrobial resistance in Ureaplasma species. J Antimicrob Chemother. 2019;74(11):3123-3131.
Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and Mycoplasma hominis, Ureaplasma urealyticum, and Ureaplasma parvum from the genitourinary tract. Manual of Clinical Microbiology. 2023;12th Edition:1115-1132.
Zhang N, Wang R, Li X, et al. Are Ureaplasma urealyticum and Ureaplasma parvum associated with adverse pregnancy outcomes? A prospective cohort study. Front Cell Infect Microbiol. 2022;12:875432.
Pereyre S, Sirand-Pugnet P, Beear-Leclere C, et al. Life without a cell wall: structural and genomic adaptations of the Mollicutes. Nat Rev Microbiol. 2016;14(8):513-524.
Sprong T, van der Zaag IH, van Kuppevelt TH, et al. Pathogenesis of Ureaplasma urealyticum in neonatal respiratory distress. Rev Med Microbiol. 2020;31(2):67-74.