MicroByte - Pathogen Series: Mycobacterium tuberculosis —Pathogen with Ancestors from the Dinosaur Era
History and Naming
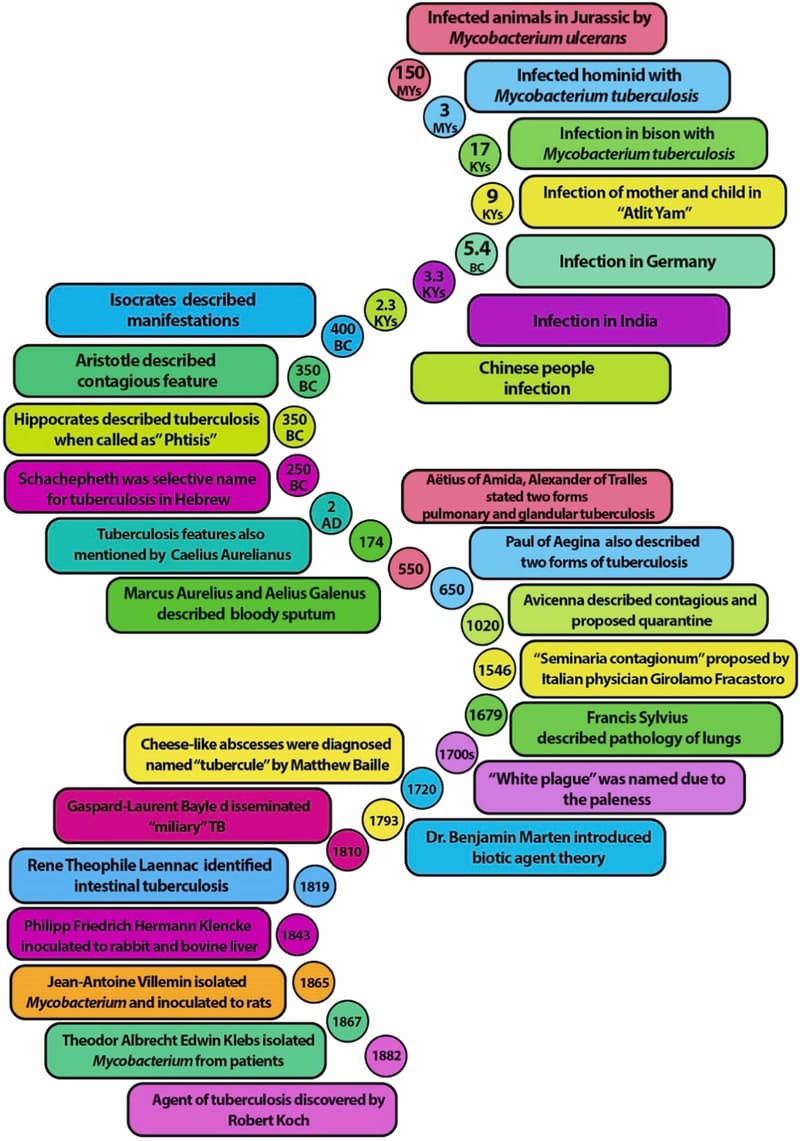
The Mycobacterium genus has existed on Earth long before humans. It is believed that one of its species, Mycobacterium ulcerans, infected animals during the Jurassic era. It is speculated that the first infection in hominid hosts occurred around 3 million years ago in East Africa. There is evidence of human infections based on DNA , tracing back approximately 15,000 to 20,000 years. The earliest documented cases date to about 3,300 years ago in India and 2,300 years ago in China.
Over time, the disease has been known by various names across the world, such as “king’s evil,” morbus regius or mal du roi, “phthisis,” “schachepheth,” and “white plague,” often referring to its fatal, contagious nature or symptoms like anemia and paleness. Because it frequently affected young adults, it was also called “the robber of youth” and “captain of all these men of death.”
In 1793, Scottish pathologist Matthew Baillie identified lung abscesses, referring to them as “tubercles,” meaning nodules. Observations of disease spread to other organs also led to the recognition of extrapulmonary tuberculosis. The disease was first named “tuberculosis” by Johann Lucas Schönlein. In 1843, Philipp Friedrich Hermann Klencke conducted experiments by inoculating material from miliary (seed-like) lung lesions into rabbit and bovine liver to better understand disease pathogenesis. Following this, several scientists worked to isolate and characterize the causative organism.
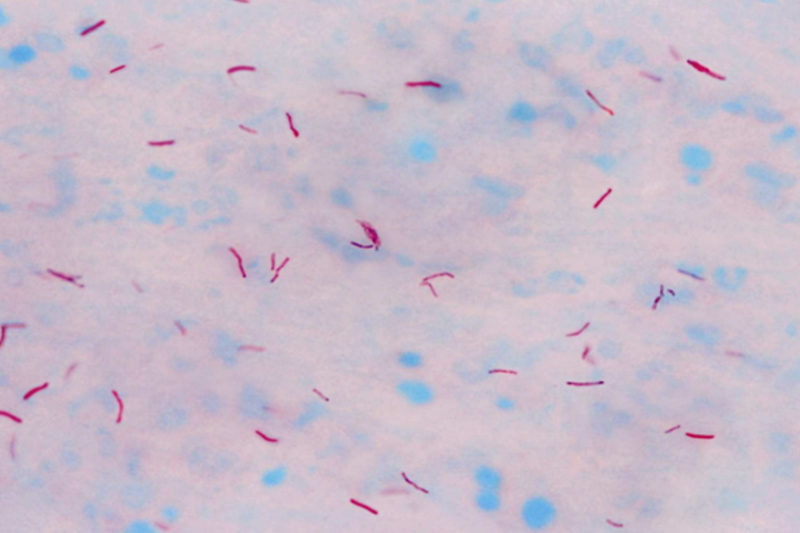
A major breakthrough came when Robert Koch successfully isolated, identified, and cultivated the bacterium responsible for tuberculosis using animal models. He initially named it “Tuberkelvirus,” later renaming it Mycobacterium tuberculosis. Koch was also the first to visualize the organism under a microscope. After unsuccessful staining attempts, he developed a new staining method, later refined by Franz Ziehl and Friedrich Neelsen in 1885, now known as the Ziehl-Neelsen (acid-fast) stain. Koch also successfully cultured the bacterium using media containing cow or sheep serum. For his work, he was awarded the Nobel Prize in 1905. This discovery marked a turning point, as tuberculosis, once thought to be a hereditary disease, was proven to be caused by a bacterium. This identification paved the way for drug development and effective treatment, ultimately making tuberculosis a curable disease.
Transmission
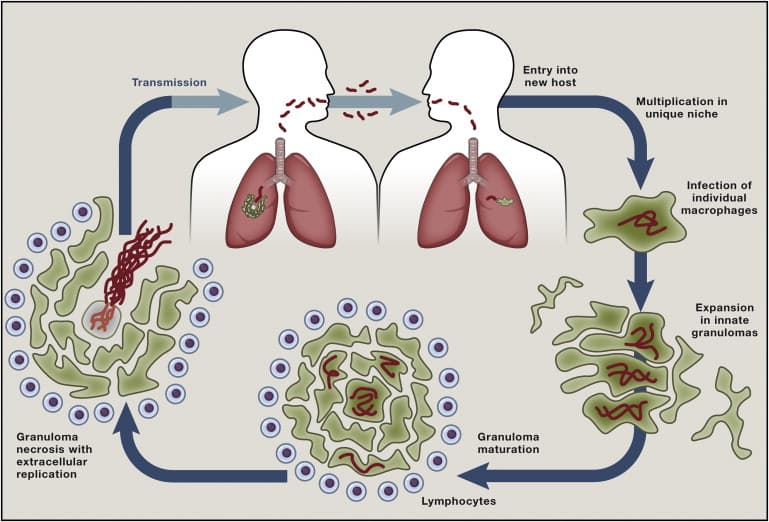
Mycobacterium tuberculosis can be transmitted through several routes, including entry of the pathogen via wounds or, rarely in the modern world, through ingestion of contaminated milk. However, one of the most common routes of transmission is through inhalation of aerosolized droplets containing the pathogen, released by an infected person when they cough, sneeze, or speak.
Pathogenesis
After inhalation of droplets containing the pathogen, M. tuberculosis(M.tb) becomes deposited in the air sacs (alveoli) of the lungs. In response to this invasion, host immune cells such as monocytes and macrophages are recruited. The bacteria are then internalized by macrophages.
There are several possible fates of the internalized M.tb:
1. It may be killed by the macrophages.
2. It may survive and kill the macrophages.
The fittest M.tb, capable of manipulating and evading host immune responses, multiply within the macrophages. However, the host immune system recognizes the pathogen and attempts to localize the infection within the lung tissue. Immune cells, including lymphocytes, are deployed to the site of infection, and infected macrophages become surrounded by monocytes, leading to the formation of solid granulomas-typical feature of tuberculosis.
Within these granulomas, the pathogen can persist and evade immune recognition and destruction. Over time, the bacteria may be released from the granulomas/lesions, leading to progression to symptomatic disease and potential transmission to new hosts. At this stage, the pathogen can also disseminate into the bloodstream and spread to other organs, such as lymph nodes, the genitourinary system, joints and bones, kidneys, and the meninges, causing extrapulmonary tuberculosis.
Symptoms and Diagnosis
The symptoms of tuberculosis are non-specific and include cough, fever, weight loss, night sweats, and malaise. Therefore, it can be challenging for clinicians to diagnose tuberculosis. Patient history is usually taken as part of the initial assessment, including information about past TB infection, recent travel, immunosuppression, and recent exposure to an infected person.
Clinicians may recommend a chest X-ray to check for lesions (solid granulomas) in the lung tissue, which can indicate past or latent infection. Microbiological investigation is the conventional approach for diagnosing active infection. Samples such as sputum, lung tissue, or cerebrospinal fluid (CSF) are collected for bacterial culture or microscopic detection of the pathogen. M. tuberculosis is a slow-growing bacterium and typically takes about two weeks to grow in culture media. Acid-fast staining is commonly performed to identify the pathogen microscopically. Due to the slow growth of the bacterium in culture and the lack of standardized procedures for microscopic examination, molecular detection methods such as nucleic acid amplification tests and lateral flow assays, are often used for the rapid detection of Mycobacterium tuberculosis, alongside conventional tests.
Antibiotic resistance in M. tuberculosis is increasing at an alarming rate, which reduces the effectiveness of standard treatments. Therefore, in addition to diagnostic tests, drug susceptibility testing is performed to identify the most effective antibiotics. Resistance is also routinely monitored throughout the course of treatment.
Treatment
Tuberculosis is treatable and curable if it is diagnosed early and the appropriate treatment is given and followed for the recommended duration. Treatment is also provided to asymptomatic patients to prevent progression to active disease. Such preventive treatment typically lasts for a minimum of three months and may include a combination of medications such as isoniazid, rifampin, and/or rifapentine.
In cases of active infection, the duration of treatment may be four, six, or nine months, depending on the regimen. Combination therapy is used and may include drugs such as ethambutol, isoniazid, moxifloxacin, rifampin, rifapentine, and pyrazinamide.
In cases of drug-resistant tuberculosis, there is a higher risk of treatment failure, and therefore prolonged treatment regimens, lasting up to 18 to 21 months are required. These regimens include first-line drugs for susceptible bacteria, as well as second-line and newer or repurposed agents to target multidrug-resistant strains. These may include delamanid, bedaquiline, pretomanid, linezolid, amoxicillin-clavulanate, meropenem-clavulanate, imipenem-cilastatin, cotrimoxazole, and macrolides.
Prevention
Since the development of the BCG vaccine, a live attenuated vaccine derived from M. bovis in 1974, it has been administered to infants and young children to help prevent infection with M. tuberculosis. Although it is effective in children, its protective effect wanes over time and offers limited protection when administered to adults.
Due to the rapid emergence of mutations and antibiotic resistance, the development of more effective vaccines and drugs is still ongoing. It is advisable to avoid close contact with individuals with confirmed tuberculosis, especially for those who are immunocompromised.
Microbe profile
Shape: Rod shaped
Spore formation: No
Biofilm formation: Yes
Oxygen requirement: Obligate anaerobe
Optimal temperature: 37C
Optimal pH: 6.4–7.0
Nutrient usage/Laboratory culture media: Lowenstein-Jensen (LJ)
Taxonomic classification
Domain: Bacteria
Kingdom: Bacillati
Phylum: Actinomycetota
Class: Actinomycetes
Order:Mycobacteriales
Family:Mycobacteriaceae
Genus: Mycobacterium
Species:M. tuberculosis
-Khushi.C
Also Read: The MicroByte - Pathogen Series: Fusobacterium nucleatum - A Prolific Pathobiont
References
Tobin EH, Tristram D. Tuberculosis Overview. [Updated 2024 Dec 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441916/
Yang, J., Zhang, L., Qiao, W., & Luo, Y. (2023). Mycobacterium tuberculosis: Pathogenesis and therapeutic targets. MedComm, 4(5), e353. https://doi.org/10.1002/mco2.353
Cambier, C. J., Falkow, S., & Ramakrishnan, L. (2014). Host evasion and exploitation schemes of Mycobacterium tuberculosis. Cell, 159(7), 1497–1509. https://doi.org/10.1016/j.cell.2014.11.024
Mousavi-Sagharchi, S. M. A., Ghorbani, A., Meskini, M., & Siadat, S. D. (2025). Historical examination of tuberculosis; from ancient affliction to modern challenges. Journal of infection and public health, 18(3), 102649. https://doi.org/10.1016/j.jiph.2024.102649