The Pathobyte Series: Mycobacterium avium: Birds and Beyond
Mycobacterium avium is a slow-growing, weakly Gram-positive bacillus capable of causing a wide array of human illnesses. Driven by an advanced arsenal of intracellular survival mechanisms, it effortlessly evades host immunity, spreading silently through environmental exposure to contaminated water and soil. Infections range from localized cervical lymphadenitis to life-threatening systemic conditions, including chronic pulmonary disease and disseminated bacteremia. Accurate diagnosis leverages classic acid-fast staining and modern tools like molecular testing. While treatment typically requires prolonged multidrug antibiotic therapy with targeted macrolides, robust prevention relies heavily on maintaining clean household water systems and preserving immune health.
What is Mycobacterium avium?
Mycobacterium avium is a slow-growing environmental bacterium that belongs to the non-tuberculous mycobacteria (NTM) group. It is commonly found in soil, water systems, dust, and natural environments. In humans, it can cause lung disease, lymph node infections, and disseminated infections, particularly in people with weakened immune systems or chronic lung conditions.
Unlike Mycobacterium tuberculosis, M. avium is generally not considered highly contagious between people. Most infections are associated with environmental exposure rather than person-to-person spread. Diagnosis usually requires imaging studies and laboratory culture, while treatment often involves long-term combination antibiotic therapy.
How was Mycobacterium avium named? What is its History?
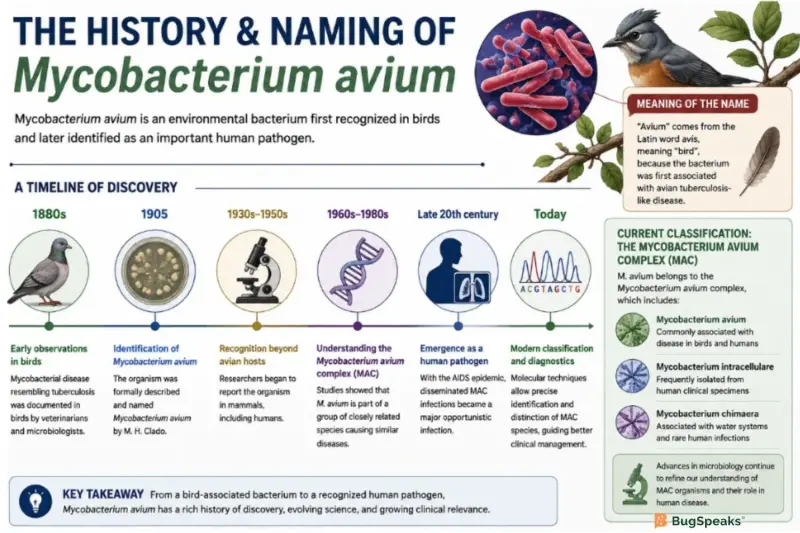
Mycobacterium avium was originally identified in birds and later recognized as a human pathogen. The term “avium” comes from the Latin word avis, meaning bird, because the bacterium was first associated with avian tuberculosis-like disease.
Over time, microbiologists discovered that M. avium belongs to a broader group called the Mycobacterium avium complex (MAC), which includes closely related species such as Mycobacterium intracellulare. Advances in molecular diagnostics during the late 20th century improved the classification and differentiation of MAC organisms.
Interest in MAC infections increased significantly during the HIV/AIDS epidemic, when disseminated M. avium infections became a major opportunistic infection in severely immunocompromised individuals. Today, MAC-related pulmonary disease is increasingly recognized in older adults and people with structural lung disease.
What Diseases Does Mycobacterium avium Cause?
Mycobacterium avium primarily causes pulmonary disease, disseminated infection, and lymphadenitis. Disease severity varies depending on immune status and underlying health conditions.
Common Conditions Associated with M. avium
How Does Mycobacterium avium Cause Disease? (Pathogenesis)
Mycobacterium avium causes disease by surviving inside immune cells, resisting intracellular destruction, and establishing persistent infection in susceptible hosts. Disease progression depends on both bacterial survival mechanisms and the immune status of the infected individual.
Unlike many extracellular bacteria, M. avium is an intracellular pathogen. After entering the body most commonly through inhalation of aerosolized particles, it is engulfed by macrophages, which are immune cells responsible for destroying microbes. However, M. avium possesses several cellular features that allow it to survive within these cells rather than being eliminated.
What Are the Symptoms of Mycobacterium avium Infection?
Symptoms depend on the site of infection and the immune status of the individual.
Pulmonary Disease Symptoms
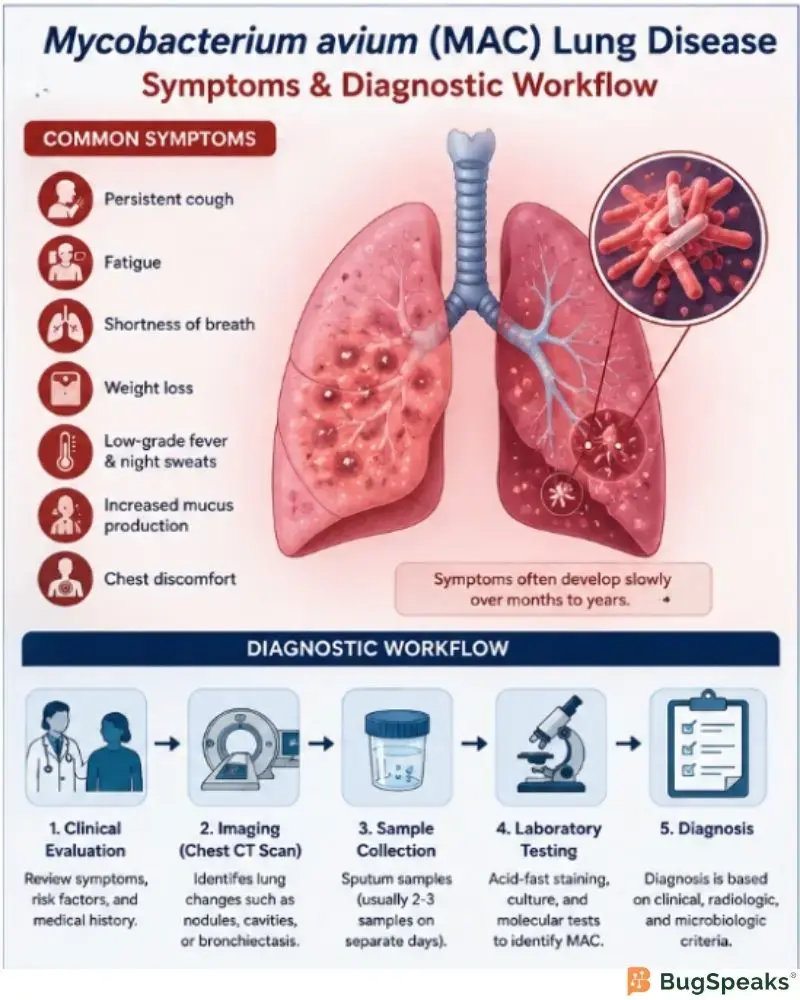
Pulmonary MAC disease often develops slowly over months or years.
Common symptoms include:
Persistent cough
Fatigue
Shortness of breath
Weight loss
Low-grade fever
Night sweats
Chest discomfort
Increased mucus production
Disseminated Infection Symptoms
In disseminated disease, the bacterium spreads through the bloodstream.
Symptoms may include:
Persistent fever
Severe fatigue
Weight loss
Diarrhea
Abdominal pain
Enlarged liver or spleen
Anemia
Lymph Node Infection Symptoms
Children with cervical lymphadenitis may develop:
Swollen lymph nodes in the neck
Mild tenderness
Skin discoloration over lymph nodes
How Is Mycobacterium avium Transmitted?
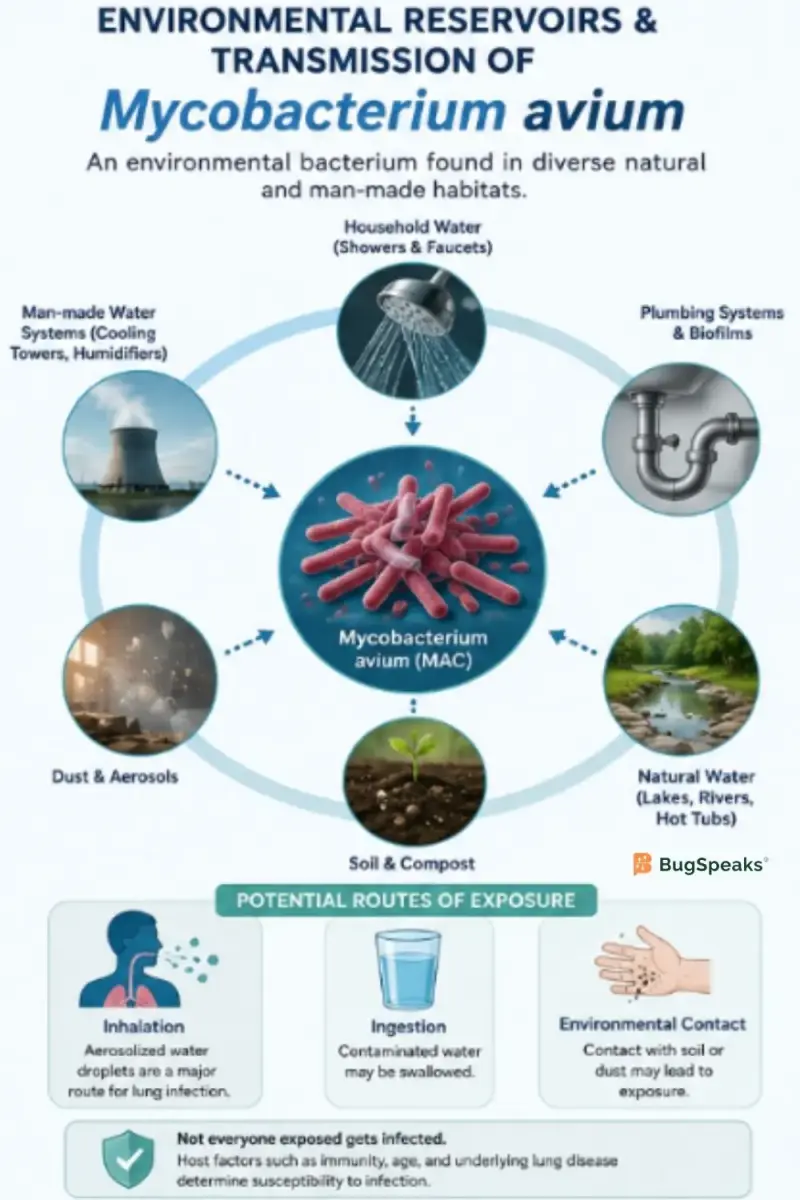
Mycobacterium avium is mainly acquired through environmental exposure. Current evidence does not support routine person-to-person transmission in most settings.
Common Environmental Sources
The bacterium has been isolated from:
Household plumbing systems
Showerheads
Natural water bodies
Soil and dust
Aerosolized water particles
Potential Routes of Exposure
Researchers believe inhalation of aerosolized bacteria is a major pathway in pulmonary disease. However, exposure alone does not necessarily lead to illness. Host susceptibility plays a major role.
Risk Factors
People at higher risk include:
Individuals with chronic obstructive pulmonary disease (COPD)
People with bronchiectasis
Individuals with cystic fibrosis
Advanced HIV/AIDS patients
Organ transplant recipients
Older adults
How is Mycobacterium avium diagnosed?
Diagnosis requires a combination of clinical evaluation, imaging, and laboratory testing. Because MAC organisms can colonize airways without causing disease, laboratory detection alone is insufficient for diagnosis.
Diagnostic Methods
Diagnostic Challenges
Diagnosis can be delayed because symptoms resemble other respiratory conditions, including tuberculosis and chronic bronchitis. MAC organisms also grow slowly in laboratory cultures, sometimes requiring several weeks for confirmation.
What Treatments Are Used for Mycobacterium avium Infection?
Treatment usually involves prolonged multidrug antibiotic therapy. Management depends on disease severity, infection site, and patient health status.
Standard Treatment Approach
Pulmonary MAC disease is commonly treated using combinations of:
Macrolides (azithromycin or clarithromycin)
Ethambutol
Rifampin or rifabutin
Therapy often continues for at least 12 months after cultures become negative.
Severe or Disseminated Disease
In advanced disease, additional antibiotics such as aminoglycosides may be required.
Treatment Challenges
Close monitoring is important because long-term therapy may affect liver function, vision, or hearing, depending on the medications used.
How Can Mycobacterium avium Infection be Prevented?
Prevention focuses on reducing exposure risk in susceptible individuals and maintaining immune health.
Prevention Strategies
Maintain clean household water systems
Reduce exposure to aerosolized water in high-risk settings
Follow HIV treatment protocols to preserve immune function
Manage chronic lung diseases appropriately
Use sterile medical equipment in healthcare environments
Healthcare Prevention
In individuals with advanced HIV infection, preventive antibiotic therapy may be considered under clinical guidance.
Currently, no vaccine specifically targets Mycobacterium avium infection.
What Is the Microbe Profile of Mycobacterium avium?
Taxonomic Classification
Why Is Mycobacterium avium Clinically Important?
Mycobacterium avium is clinically important because it represents one of the most common non-tuberculous mycobacterial pathogens worldwide. Improved imaging and laboratory techniques have increased recognition of MAC-associated disease in both immunocompromised and immunocompetent populations.
Researchers continue to study why some individuals develop progressive disease while others remain asymptomatic despite environmental exposure.
Reference
Falkinham JO III. Environmental sources of nontuberculous mycobacteria. Clin Chest Med. 2015.
Daley CL, et al. Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Clin Infect Dis. 2020.
Griffith DE, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007.
Johansen MD, et al. Mycobacterium avium complex and the lung: a review. Clin Microbiol Rev. 2020.
Winthrop KL, et al. Pulmonary nontuberculous mycobacterial disease prevalence and clinical features. Am J Respir Crit Care Med. 2010.
Henkle E, Winthrop KL. Nontuberculous mycobacteria infections in immunosuppressed hosts. Clin Chest Med. 2015.
Haworth CS, et al. British Thoracic Society guidelines for management of non-tuberculous mycobacterial pulmonary disease. Thorax. 2017.
Ratnatunga CN, et al. The rise of non-tuberculous mycobacterial lung disease. Front Immunol. 2020.
Bermudez LE, Sangari FJ, Kolonoski P, Petrofsky M, Goodman J. The Mycobacterium avium complex: pathogenesis and virulence factors. FEMS Microbiol Rev. 2004;28(1):77–90.