The Pathobyte Series: Coxiella burnetii-Tracking the Agent of Q Fever
Coxiella burnetii is a highly infectious, globally distributed intracellular bacterium that serves as the causative agent of Q fever. Primarily residing in domestic ruminants like sheep and cattle, the pathogen sheds heavily during parturition and spreads to humans via airborne aerosols. Infection manifests as an acute flu-like illness, pneumonia, or hepatitis, which can progress into fatal chronic endocarditis if left untreated. Diagnosis relies on PCR assays and serological screening. Acute cases are treated with doxycycline, whereas chronic infections necessitate an extended doxycycline-hydroxychloroquine regimen. Prevention focuses on farm biosecurity, milk pasteurization, and targeted vaccination under a coordinated One Health framework.
Introduction
Coxiella burnetii is a highly infectious, obligate intracellular bacterium renowned for its remarkable environmental stability and its role as the causative agent of Q fever. First identified in the 1930s, this pathogen remains a significant public health concern due to its zoonotic nature, meaning it primarily circulates in animals but can readily infect humans. Found globally with the notable exception of New Zealand, C. burnetii maintains a vast reservoir among domestic ruminants like sheep, goats, and cattle.
Understanding this microorganism is crucial for clinicians, agricultural workers, and public health officials alike. Its exceptionally low infectious dose means that inhaling a single organism can be sufficient to cause infection. Because its clinical presentation mimics common flu-like illnesses or atypical pneumonias, it frequently goes undiagnosed, leaving some patients vulnerable to severe, life-altering chronic complications like endocarditis.
What is Coxiella burnetii?
Diseases Caused
The primary pathology associated with this organism is Q fever (Query fever). In humans, this manifests in two distinct clinical phases: acute Q fever, which typically presents as a self-limiting febrile illness, pneumonia, or hepatitis, and chronic Q fever, a persistent, severe infection that most commonly manifests as culture-negative endocarditis in individuals with pre-existing heart valve defects or compromised immune systems.
Public Health Significance
C. burnetii is classified as a Select Agent and a potential bioweapon (Category B bioterrorism agent) by the Centers for Disease Control and Prevention (CDC) due to its extreme infectivity via aerosols and its resilience to environmental degradation. A single outbreak can disrupt agricultural economies and overwhelm local healthcare systems.
Global Prevalence
The bacterium exhibits a cosmopolitan distribution, endemic in almost every country where livestock is raised. The epidemiology varies by region; for instance, major outbreaks have been documented in the Netherlands, while endemic pockets present continuous exposure risks across rural landscapes in the United States, Europe, and Australia.
History and Naming
The history of Coxiella burnetii centers on its independent discovery in Australia and the United States during the late 1930s, resolving the mystery of an unexplained febrile illness among abattoir workers.
Discovery and Scientists Involved
The disease was first recognized in 1935 by Edward Holbrook Derrick in Brisbane, Queensland, Australia, among workers in a local slaughterhouse. Because the cause of the febrile illness was unknown, Derrick dubbed it "Query fever" (Q fever).
In 1937, Frank Macfarlane Burnet and Mavis Freeman isolated the causative organism from patient samples sent by Derrick, identifying it as a rickettsia-like bacterium. Concurrently, Herald Rea Cox and Gordon Davis isolated the same organism from Rocky Mountain wood ticks (Dermacentor andersoni) in Montana, USA.
Origin of the Name
The genus name Coxiella honors Herald Rea Cox for his pioneering work in isolating and characterizing the bacterium. The species name burnetii recognizes Sir Frank Macfarlane Burnet for his fundamental contributions to understanding its biological properties.
Historical Outbreaks and Microbiology Importance
Historically, Q fever was heavily associated with military campaigns, notably affecting Allied and Axis troops in the Mediterranean basin during World War II (known then as "Balkan influenza"). In modern microbiology, C. burnetii served as a paradigm-shifting organism; it challenged early definitions of bacteria by demonstrating a spore-like environmental stability while remaining dependent on a eukaryotic host cell for replication.
Microbe Profile
Taxonomic Classification
Pathogenesis
Pathogenesis refers to the biological mechanisms and sequence of cellular events by which Coxiella burnetii invades a host organism, survives intracellular defenses, and establishes infection.
Virulence Factors
The primary virulence factor of C. burnetii is its Lipopolysaccharide (LPS).
Phase I Variant: Smooth LPS found in nature; highly infectious and capable of shielding the bacterium from host immune recognition.
Phase II Variant: Rough LPS generated after repeated laboratory passage; non-infectious to immunocompetent hosts.
Type IVB Secretion System (T4BSS): A macromolecular syringe used by the bacterium to inject effector proteins into the host cytoplasm, manipulating host cell functions to prevent apoptosis and orchestrate vacuole development.
Host Cell Invasion and Intracellular Survival
C. burnetii primarily targets eukaryotic phagocytes, such as macrophages and monocytes. Upon entering the host cell via receptor-mediated phagocytosis, the bacterium does not evade the lysosome. Instead, it thrives within the Coxiella-containing vacuole (CCV), an acidic, hydrolytic compartment formed by the fusion of the phagosome with lysosomes. The low pH serves as the precise environmental cue that triggers the metabolic activation of the pathogen.
Replication Cycle and Biphasic Developmental Cycle
The bacterium transitions through a distinct biphasic life cycle:
Small Cell Variant (SCV): The metabolically inactive, condensed form found in the environment. It is resistant to heat, desiccation, and chemical disinfectants. The SCV infects the host macrophage.
Large Cell Variant (LCV): Inside the acidic CCV, the SCV differentiates into the larger, metabolically active, and replicating LCV. After multiple rounds of binary fission, the LCVs condense back into SCVs before the host cell lyses, releasing the bacteria to infect neighboring cells.
Mechanism of Disease: Acute vs. Chronic
In acute infection, the rapid replication of C. burnetii and the subsequent cell-mediated immune response provoke localized inflammation, leading to tissue damage in the lungs (pneumonia) or liver (granulomatous hepatitis).
In chronic infection, a failure of the host's cell-mediated immunity allows the pathogen to persist long-term. The bacteria colonize damaged cardiac valves or vascular endothelium, where persistent low-grade inflammation leads to progressive valve destruction and fibrosis.
Transmission
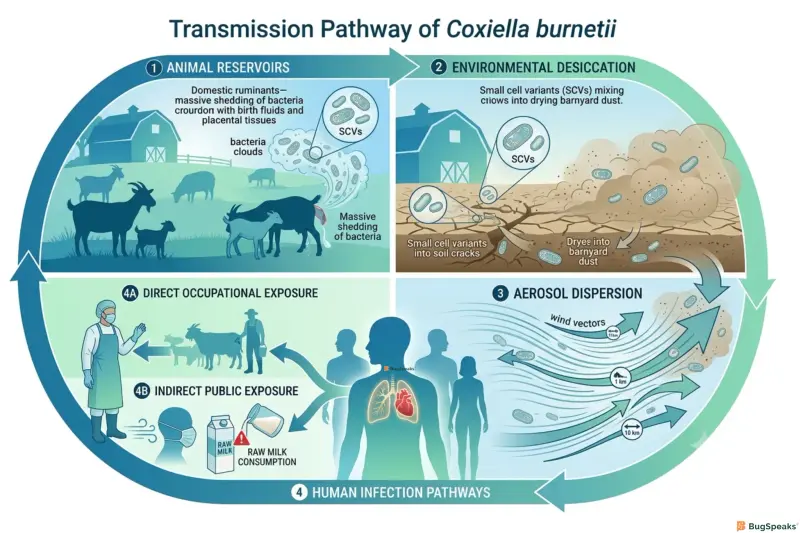
Transmission encompasses the pathways through which Coxiella burnetii moves from its natural animal reservoirs to susceptible human hosts, primarily driven by airborne dissemination.
Reservoirs and Animal Hosts
The primary reservoirs are domestic ruminants: sheep, goats, and cattle. While infected animals are generally asymptomatic, the bacteria localize in the uterus and mammary glands. During parturition (birth), enormous quantities of C. burnetii (up to $10^9$ bacteria per gram of placenta) are shed into the environment via birth fluids, placenta, feces, urine, and milk.
Aerosol Transmission and Environmental Persistence
The dominant route of human infection is the inhalation of contaminated aerosols or dust. When birth fluids or excreta dry in pastures or barns, the resilient SCVs mix with dust particles. Wind currents can carry these infectious particles over significant distances—sometimes several kilometers—causing infections in individuals with no direct animal contact.
[Infected Livestock] ---> [Contaminated Placenta/Fluids] ---> [Desiccation into Dust (SCVs)]
Occupational Exposure
Certain professions carry a vastly elevated risk of exposure:
Veterinarians and veterinary technicians
Livestock farmers and ranch hands
Abattoir (slaughterhouse) workers
Laboratory researchers handling viable cultures
Rare Modes of Transmission
Ingestion: Consuming unpasteurized milk or dairy products from infected animals.
Vector-borne: Ticks serve as natural vectors maintaining the cycle in wild animal populations, but tick bites are a rare cause of human cases.
Person-to-person: Extremely rare, but documentable via blood transfusions, transplacental transmission from mother to fetus, or sexual contact.
Signs and Symptoms
Clinical manifestations describe the broad spectrum of signs (objective findings) and symptoms (subjective experiences) that present during acute or chronic Coxiella burnetii infection.
Incubation Period
The incubation period for acute Q fever typically ranges from 2 to 3 weeks (range: 14–39 days), depending significantly on the size of the initial infectious inoculum.
Acute Q Fever
Approximately 50–60% of individuals infected with C. burnetii remain asymptomatic. For those who develop symptoms, acute Q fever presents abruptly with:
High fever (often up to $40^\circ\text{C}$ or $104^\circ\text{F}$) accompanied by chills or rigors
Severe, debilitating frontal headaches (retro-orbital pain)
Profuse drenching sweats
Extreme fatigue and myalgia (muscle aches)
Non-productive cough and pleuritic chest pain (indicative of atypical pneumonia)
Nausea, vomiting, diarrhea, and abdominal pain (indicative of Q fever hepatitis)
Chronic Q Fever
Developing in less than 5% of acute cases, chronic Q fever evolves slowly over months or years. It is highly lethal if untreated.
Endocarditis: Constitutes over 70% of all chronic cases. It presents as culture-negative endocarditis, characterized by progressive heart failure, heart murmurs, splenomegaly, and clubbing of digits.
Vascular Infections: Infection of aneurysms or vascular grafts.
Osteoarticular Infections: Chronic osteomyelitis or septic arthritis.
Post-Q Fever Fatigue Syndrome (QFS): A debilitating chronic fatigue state following acute infection, characterized by headaches, arthralgia, and sleep disturbances, without ongoing bacterial replication.
Diagnosis
Diagnosis involves the systematic identification of Coxiella burnetii infection using a combination of clinical suspicion, serological profiles, and molecular assays.
Laboratory Methods
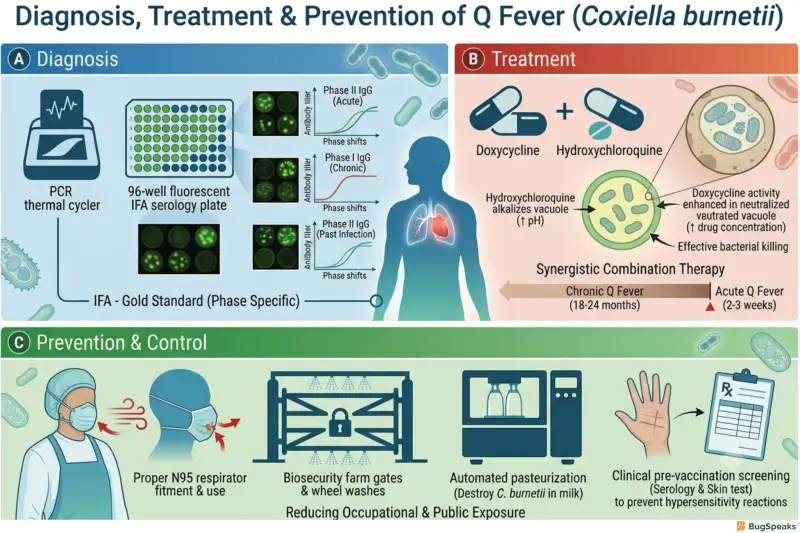
Serology (Indirect Immunofluorescence Assay - IFA): The gold standard tool. IFA measures antibody titers against Phase I and Phase II antigens.
Acute Q Fever: Characterized by a high titer of antibodies to Phase II antigen.
Chronic Q Fever: Characterized by a very high titer of IgG antibodies to the Phase I antigen.
Polymerase Chain Reaction (PCR): Highly effective during the first two weeks of acute illness before antibody titers rise. It targets specific insertion sequences like IS1111.
Enzyme-Linked Immunosorbent Assay (ELISA): Often utilized for rapid screening in epidemiological surveys.
Differential Diagnosis
Due to its non-specific symptoms, C. burnetii infection must be differentiated from:
Infections by Mycoplasma pneumoniae or Chlamydia pneumoniae
Brucellosis and Leptospirosis
Legionnaires' disease
Infective endocarditis caused by HACEK organisms or Bartonella species
Diagnostic Methodology Comparison
Treatment
Treatment consists of specific antimicrobial therapies selected to penetrate host cells and eliminate Coxiella burnetii from intracellular niches.
First-Line Antibiotics & Protocols
Acute Q Fever: The definitive treatment of choice is Doxycycline orally twice daily. For a duration of 14 days. Therapy is most effective when initiated within the first 3 days of symptom onset.
Chronic Q Fever: Requires an extended, combined regimen to alter the pH of the host vacuole and ensure bacterial clearance. The gold standard is Doxycycline combined with Hydroxychloroquine. Hydroxychloroquine raises the lysosomal pH, rendering the doxycycline bactericidal against C. burnetii.
Special Populations
Pregnant Women: Doxycycline is contraindicated due to fetal bone and dental risks. Trimethoprim/sulfamethoxazole (TMP-SMX) is recommended throughout pregnancy to prevent obstetric complications, followed by a reassessment postpartum.
Children: Short courses (14 days) of doxycycline are safe and remain first-line for acute disease in pediatric populations under clinical guidelines.
Treatment Protocol Summary
Prevention
Prevention comprises biosecurity, hygiene, and physical containment protocols aimed at minimizing human and animal exposure to infectious Coxiella burnetii shedding.
Farm Management and Biosecurity
Safe Handling of Livestock: Isolating pregnant animals during lambing or calving phases to prevent widespread pasture contamination.
Disposal of Birth Tissues: Incineration or deep burial of placentas, aborted fetuses, and bedding materials.
Sanitation: Using validated chemical disinfectants (e.g., 0.5% sodium hypochlorite, 2% formaldehyde) on contaminated surfaces, noting that standard alcohol rubs are insufficient against SCVs.
Personal and Occupational Precautions
Personal Protective Equipment (PPE): Veterinarians, farm workers, and laboratory personnel should wear properly fitted N95 or higher particulate respirators, gloves, and protective coveralls when handling birth tissues or cleaning animal housing.
Milk Pasteurized Consumption: Mandatory pasteurization of commercial milk supplies destroys C. burnetii, protecting general consumers from oral exposure.
Vaccines
Definition
Vaccination introduces specific antigenic components to induce protective cell-mediated immunity against future Coxiella burnetii exposures.
Existing Vaccines & Availability
An effective phase-I whole-cell inactivated vaccine known as Q-Vax is manufactured and routinely utilized in Australia for individuals in high-risk occupations.
Limitations and Administration Protocols
Q-Vax is not widely available globally (including the US and Western Europe) due to strict licensing constraints and safety profiles. The vaccine can trigger severe local or systemic hypersensitivity reactions (sterile abscesses, severe granulomas) in individuals who have had prior unrecognized exposure to C. burnetii. Consequently, pre-vaccination screening consisting of a detailed medical history, a skin hypersensitivity test, and a serological blood test is mandatory before administration.
Current Research
Current research is actively focused on developing next-generation subunit vaccines, recombinant antigen formulations, and DNA vaccines that convey protection without inducing hypersensitivity reactions, potentially paving the way for wider global adoption.
Control Measures
Definition
Control measures represent the institutional, veterinary, and environmental regulatory framework designed to identify, contain, and suppress active outbreaks of Q fever.
One Health Approach
Because C. burnetii crosses boundaries between wildlife, domestic livestock, and human populations, managing it demands a coordinated One Health approach. This integrates veterinary diagnostics, human epidemiologic tracking, and environmental monitoring to prevent zoonotic spillover.
Reference
Centers for Disease Control and Prevention (CDC). (2022). Q Fever: Epidemiology and Clinical Manifestations. U.S. Department of Health and Human Services.
Derrick, E. H. (1937). "Q" fever, a new clinic entity: Clinical features, diagnosis and laboratory investigation. Medical Journal of Australia, 2(8), 281-299.
Eldin, C., Mélenotte, C., Mediannikov, O., Badiaga, S., Million, M., Edouard, S., Pradines, B., & Raoult, D. (2017). From Q Fever to Coxiella burnetii Infection: a Paradigm Shift. Clinical Microbiology Reviews, 30(1), 115-190.https://doi.org/10.1128/CMR.00045-16
Kersh, G. J. (2022). Antimicrobial resistance in Coxiella burnetii. ASM Journals: Antimicrobial Agents and Chemotherapy, 66(4), e02111-21.
Maurin, M., & Raoult, D. (1999). Q fever. Clinical Microbiology Reviews, 12(4), 518-553.
World Health Organization (WHO). (2019). Zoonotic Diseases: Prevention and Management of Q Fever Outbreaks. WHO Global Infectious Hazards Profile.
van der Hoek, W., Dijkstra, F., Schimmer, B., Schneeberger, P. M., Vellema, P., Wijkmans, W. M., ... & Notermans, D. W. (2010). Q fever in the Netherlands: an update on the epidemiology and control measures. Eurosurveillance, 15(12), 19520.