The Pathobyte Series Corynebacterium diphtheriae: The Unseen Architect of Diphtheria
Corynebacterium diphtheriae is a pathogenic, Gram-positive bacterium primarily responsible for diphtheria, a severe and potentially fatal infection characterized by a thick grey coating in the throat and systemic organ damage. This bacterium is exceptionally dangerous because it produces a potent exotoxin that inhibits protein synthesis in human cells, leading to tissue death, airway obstruction, and heart or nerve failure. Fortunately, diphtheria is highly preventable through the widespread use of the diphtheria vaccine (often administered as DTaP or Tdap), which has reduced the incidence of the disease by over 90% globally since the mid-20th century.
What is Corynebacterium diphtheriae?
Corynebacterium diphtheriae is a non-motile, non-spore-forming, aerobic Gram-positive bacillus known for its unique "club-shaped" appearance under the microscope. While the genus Corynebacterium contains many species that are harmless inhabitants of human skin and mucous membranes, C. diphtheriae stands out as a major human pathogen.
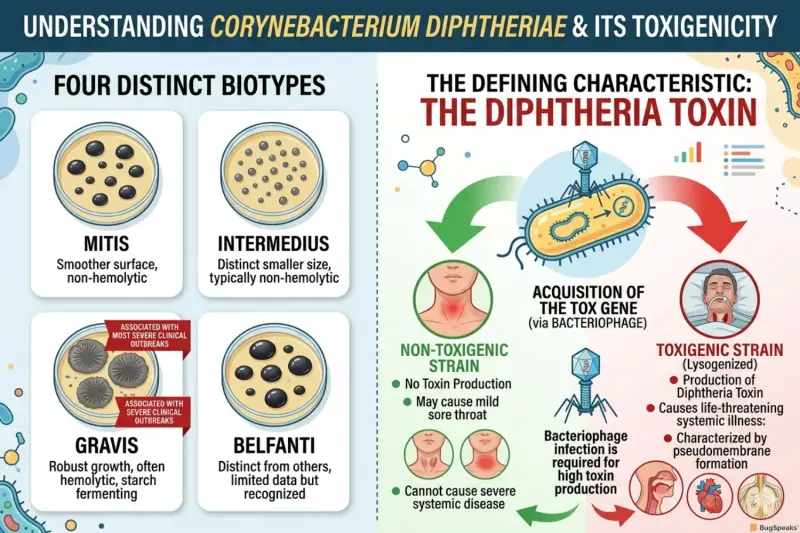
The bacterium is categorized into four distinct biotypes based on its colony morphology and biochemical properties: mitis, intermedius, gravis, and belfanti. While all four can cause disease, the "gravis" biotype is historically associated with the most severe clinical outbreaks. The most defining characteristic of this organism is not its growth pattern, but its ability to harbor a specific virus, a bacteriophage that carries the genetic code for the diphtheria toxin. Without this toxin, the bacterium may cause a mild sore throat, but it cannot cause the life-threatening systemic illness known as diphtheria.
How was Corynebacterium diphtheriae discovered and named?
Corynebacterium diphtheriae was first identified in 1883 by Edwin Klebs, and its role as the causative agent of diphtheria was confirmed a year later by Friedrich Löffler, leading to its historical nickname, the "Klebs-Löffler bacillus." The name reflects both its appearance and the pathology it creates: Coryne is derived from the Greek word for "club," describing its swollen ends, while diphtheriae comes from the Greek diphthera, meaning "leather" or "hide," referring to the tough, leathery membrane it forms in the throat of victims.
The discovery was a landmark in microbiology because it was one of the first instances where scientists proved that a bacterium could cause systemic damage through a secreted poison (toxin) rather than just through local tissue invasion. In 1888, Emile Roux and Alexandre Yersin demonstrated that filtered broth from a C. diphtheriae culture containing no live bacteria could still kill laboratory animals, proving the existence of the diphtheria toxin. This discovery paved the way for the development of the first antitoxins and vaccines.
How does Corynebacterium diphtheriae cause disease?
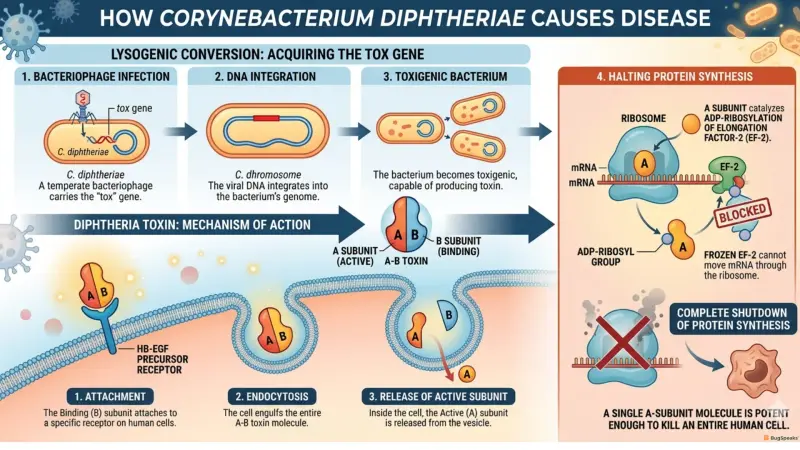
Corynebacterium diphtheriae causes disease primarily through the production of a lethal exotoxin that enters the bloodstream and halts the production of proteins within host cells. This process begins with "lysogenic conversion," where a specific virus called a bacteriophage integrates its DNA (the tox gene) into the bacterium's genome. If the bacterium is "toxigenic," it begins secreting the toxin at the site of infection.
The diphtheria toxin is an "A-B toxin." The B (Binding) subunit attaches to a receptor on the surface of human cells (specifically the heparin-binding epidermal growth factor precursor). Once attached, the cell swallows the toxin via endocytosis. Inside the cell, the A (Active) subunit is released. The A subunit catalyzes the ADP-ribosylation of Elongation Factor-2 (EF-2), a protein essential for moving mRNA through the ribosome. By "freezing" EF-2, the toxin completely shuts down protein synthesis. A single molecule of the A subunit is potent enough to kill an entire human cell.
How is diphtheria transmitted?
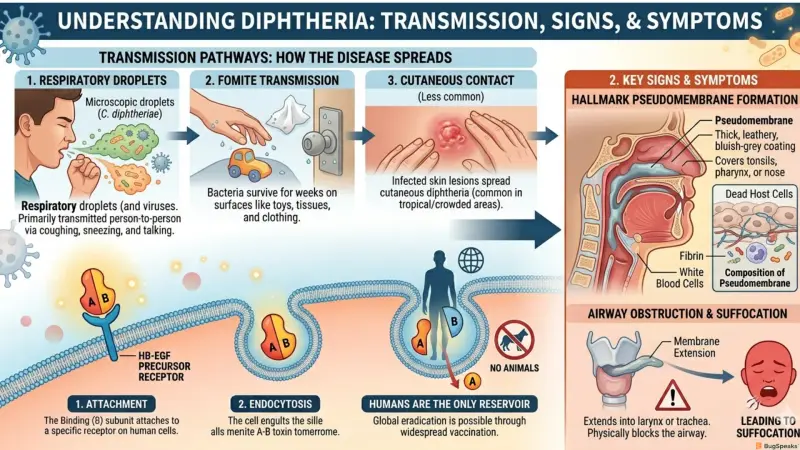
Diphtheria is primarily transmitted from person to person through respiratory droplets produced by coughing, sneezing, or even talking. When an infected individual breathes out, they release microscopic droplets containing C. diphtheriae which can then be inhaled by someone nearby. Because the bacteria can survive for several weeks on dry surfaces, transmission can also occur through fomites objects like toys, tissues, or clothing that have been contaminated by the secretions of an infected person.
In less common cases, the bacteria can be transmitted through contact with infected skin lesions, leading to cutaneous diphtheria. This form of the disease is more common in tropical climates or crowded living conditions where hygiene may be compromised. Humans are the only known reservoir for C. diphtheriae, meaning the disease does not spread from animals to humans, making global eradication a theoretically possible goal through vaccination.
What are the signs and symptoms of diphtheria?
The hallmark symptom of diphtheria is the formation of a pseudomembrane, a thick, leathery, bluish-grey coating that covers the tonsils, pharynx, or nose. This membrane is composed of dead host cells, fibrin, white blood cells, and the bacteria themselves. If the membrane extends into the larynx or trachea, it can physically block the airway, leading to suffocation.
Symptoms typically appear after an incubation period of 2 to 5 days. Initially, the patient may experience a mild fever, sore throat, and hoarseness. As the toxin spreads, the lymph nodes in the neck often swell significantly, creating a "bull neck" appearance. If the toxin enters the systemic circulation, it can lead to severe complications like myocarditis (inflammation of the heart muscle) and polyneuritis (nerve damage), which can cause paralysis.
How is diphtheria diagnosed?
Diphtheria is diagnosed through a combination of clinical observation, specifically the presence of the pseudomembrane and definitive laboratory testing to confirm the presence of C. diphtheriae and its toxin. Because the disease progresses rapidly, doctors often begin treatment based on clinical suspicion before laboratory results are finalized.
The laboratory process begins with a swab of the throat or skin lesion. The sample is cultured on specialized media, such as Löffler's serum or Tinsdale agar, which encourages the growth of Corynebacterium. Once the bacteria are isolated, it is critical to determine if the strain is "toxigenic." This is traditionally done using the Elek test, an in vitro precipitation test that detects the presence of the diphtheria toxin. Modern laboratories also use Polymerase Chain Reaction (PCR) to detect the tox gene directly, providing faster results.
How is diphtheria treated?
The treatment for diphtheria is a medical emergency and follows a two-pronged approach: neutralizing the circulating toxin and eliminating the bacteria. The most critical component is the administration of diphtheria antitoxin (DAT). Because the antitoxin can only neutralize toxins that have not yet entered human cells, it must be administered as early as possible to prevent further organ damage.
Alongside the antitoxin, patients are treated with heavy doses of antibiotics, typically Erythromycin or Penicillin G. These drugs kill the bacteria, stopping further toxin production and preventing the patient from spreading the infection to others. Patients must be kept in strict isolation until they have two consecutive negative cultures (taken 24 hours apart) to ensure they are no longer contagious.
How can diphtheria be prevented?
Diphtheria is prevented almost exclusively through widespread vaccination, which uses a toxoid, a weakened version of the diphtheria toxin that has been treated with heat or chemicals. This toxoid is non-poisonous but still triggers the body’s immune system to produce protective antibodies. If a vaccinated person is later exposed to the real bacterium, their immune system can immediately neutralize the toxin.
The CDC and WHO recommend a series of vaccinations beginning in infancy. The DTaP vaccine (Diphtheria, Tetanus, and acellular Pertussis) is given in five doses before a child reaches age six. However, immunity wanes over time, which is why booster doses are essential. Adolescents should receive the Tdap vaccine, and adults require a Td booster every 10 years to maintain protection.
Microbe Profile
Taxonomic Classification
Reference
Centers for Disease Control and Prevention (CDC). (2022). Epidemiology and Prevention of Vaccine-Preventable Diseases (The Pink Book). 14th ed. Washington, D.C.: Public Health Foundation.
Hadfield, T. L., McEvoy, P., Polotsky, Y., Tzinserling, V. A., & Belotto, A. J. (2000). The Pathology of Diphtheria. The Journal of Infectious Diseases, 181(Supplement_1), S116–S120.
World Health Organization (WHO). (2017). Diphtheria vaccine: WHO position paper – August 2017. Weekly Epidemiological Record, 92(31), 417-435.
Murphy, J. R. (1996). Corynebacterium Diphtheriae. In: Baron S, editor. Medical Microbiology. 4th edition. University of Texas Medical Branch at Galveston.
Holmes, R. K. (2000). Biology and Molecular Epidemiology of Corynebacterium diphtheriae and the Phylogeny of Diphtheria Toxin. The Journal of Infectious Diseases, 181(Supplement_1), S156–S167.